Low-grade astrocytomas (LGAs):
- Generally present with a long history of signs and symptoms
- Often non-specific and non-localizing initially
School age children may present with:
- Personality changes
- Declining academic performance
- Fatigue
- Intermittent headaches related to increased intracranial pressure (ICP)
High grade astrocytomas generally have a much shorter history of these problems prior to presentation.
Three symptoms and signs (RED flags) for increased ICP may also develop:
1. Headaches:
- Severe, progressive
- Awaken the child at night
- Associated with or relieved by morning vomiting
- Worse first thing in the morning and when the patient coughs.
2. Abducens (cranial nerve VI) palsy“False localizing” sign:
- Due to effect of increased ICP on the course of CNVI
- This nerve has a long intracranial course up the clivus and is easily affected by pressure.

The picture above shows a left lateral rectus (VI cranial nerve) palsy.
3. Papilledema
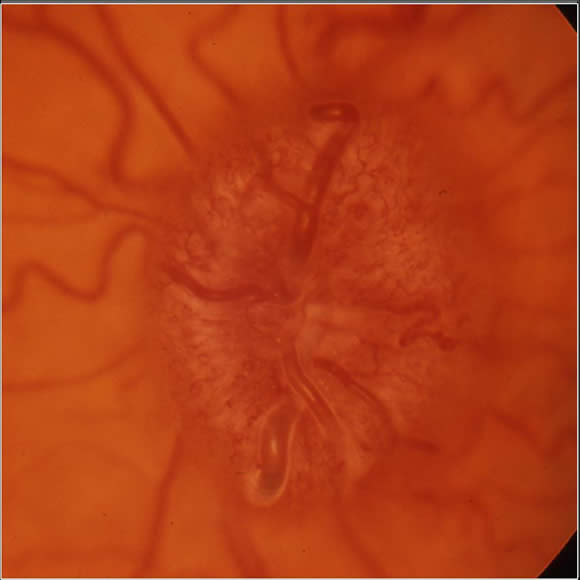
Papilledema:
This is optic disc (optic nerve head) swelling secondary to raised intracranial pressure
Results from long-standing increased ICP
Appearance on retinal examination:
- Optic disc is swollen and elevated
- There is venous engorgement (hyperemia) of the disc
- Indistinct, blurred disc margin
- Venous congestion develops with hemorrhages around the disc.
- Spontaneous venous pulsations are lost
There is classically no visual loss secondary to papilledema.
Below is an image of papilledema:
Cushing's Triad:
The combination of these three physical signs means that the raised intracranial pressure is very severe and there is impending brainstem herniation:
1. Abnormal respirations
- Change in respiratory pattern with irregular respirations
2. Hypertension
- Progressively increasing systolic blood pressure
- An increase in the difference between systolic and diastolic pressure over time
3. Bradycardia
Infant Presentation:
Infants with astrocytoma often present with non-specific problems such as:
- Irritability
- Feeding difficulties
- Failure to thrive
- Gross motor delay or regression
- Increasing head circumference, bulging fontanelles and prominent scalp veins
- Parinaud’s syndrome.
Physical findings are related to increased ICP in the dorsal midbrain:
- Paralysis of up gaze
- This vertical palsy is supranuclear, so a doll’s head maneuver may elevate the eyes, but eventually all upward gaze mechanisms fail
- Pseudo-Argyll Robertson pupils
- Pupils respond poorly to light but will constrict with accommodation
- Nystagmus
- Attempts at upward gaze often produce this phenomenon
- Upper eyelid retraction (Collier's sign)
Parinaud's may be associated with cranial nerve IV palsy, resulting in “down and out” deviation of the affected eye and often accompanied by a compensatory head tilt to the contralateral side.

As the tumor progresses, symptoms may relate directly to areas of brain involvement:
- Posterior fossa lesions are associated with:
- Ataxia
- Clumsiness
- Intention tremor
- Hemispheric tumors involving the motor cortex may cause:
- Focal motor deficits
- Seizures
- Astrocytomas of the visual pathway
often cause:
- Visual deficits