Anaplastic astrocytoma (WHO grade III) and glioblastoma multiforme (WHO grade IV) are high grade astrocytomas.
Anaplastic astrocytoma:
Macroscopic Features:
- Generally produces a discernible tumor mass
- Infiltrates into surrounding brain parenchyma and structures
Microscopic Features:
- Increased cellularity
- Nuclear atypia and mitotic activity
- Cells are enlarged, irregular and have hyperchromatic nuclei
- Vascular proliferation and necrosis are absent
Genetic Analysis:
High frequency of p53 mutation. In approximately 50% of cases there is loss of heterozygosity (LOH) on chromosome 19q. EGFR amplification is rare.
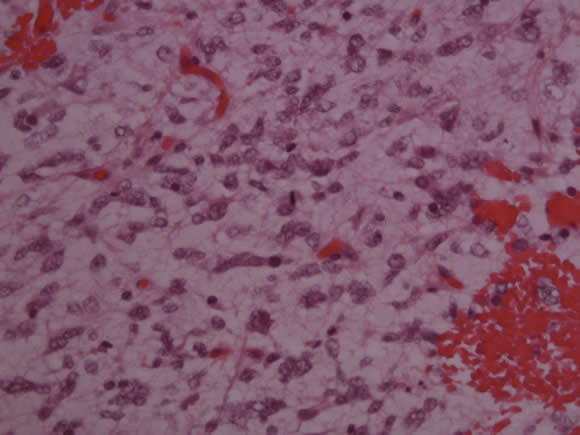
The slide below shows an anaplastic astrocytoma with moderate cellularity, nuclear atypia and a mitotic figure (center).
Glioblastoma Multiforme
Macroscopic Features:
- Often large mass lesion at the time of diagnosis.
- Intracranial mass shift.
- Can extend across myelinated structures such as the corpus callosum resulting in bilateral involvement.
- Tumor mass generally shows variable coloration, necrosis and hemorrhage.
Microscopic Features:
- Tumor shows high cellularity, nuclear pleomorphism, necrosis, microvascular proliferation and mitotic activity.
- Tumor cells are variable in appearance and can be small and undifferentiated, granular, bipolar, fusiform, or large and multinucleated.
- Infiltrative, and tumor cells accumulate in subpial, subependymal, perivascular and perineuronal regions.
- Areas of circumscribed necrosis and psudopalisading.
Genetic Analysis:
Glioblastomas in children have different genetic alteration compared with adults; 40% show p53 gene mutations and loss of heterozygosity at 17p. There is a low frequency of EGFR amplification and a high frequency of LOH on chromosome 10.
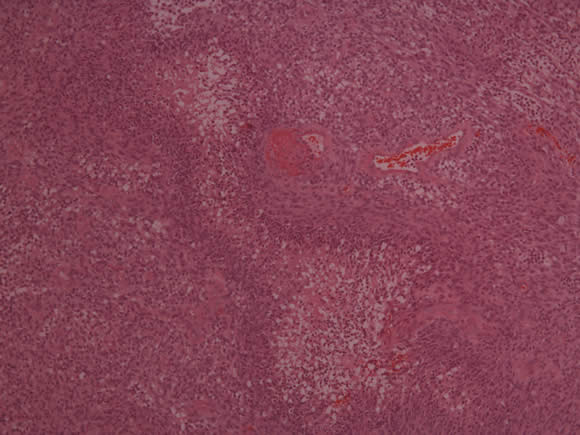
The slide below shows a glioblastoma multiforme with high cellularity, necrosis, pseudopalisading and vascular proliferation.
[P5] .