RT can be used to achieve local control, but is not generally used in children less than 5 years of age and avoided if possible in children between 5 and 10 years of age.
RT is delayed as far as possible in young children (generally by using chemotherapy) to reduce the risk significant late effects – such as neurocognitive delay.
Relapse after first line chemotherapy can be managed by using second line chemotherapy to further delay RT5.
Different techniques can be used to spare surrounding normal structures, such as stereotactic radiotherapy, IMRT and protons.
For conventional 3-D conformal RT plans, a portal/block margin of approximately 1.0 to 1.5 cm is often used. Adequate immobilization is essential.
RT doses are generally in the range of 45 Gy to 54 Gy in 180 cGy fraction size.
NF1 Patients with optic pathway glioma : have a better overall prognosis, but:
- Less likely to respond to RT
- Higher risk of developing late effects such as:
- Second cancers
- Endocrinopathy
- Developmental and neurocognitive problems
- Vasculopathy
- Moya-moya
- RT induced cerebral artery aneurysm6
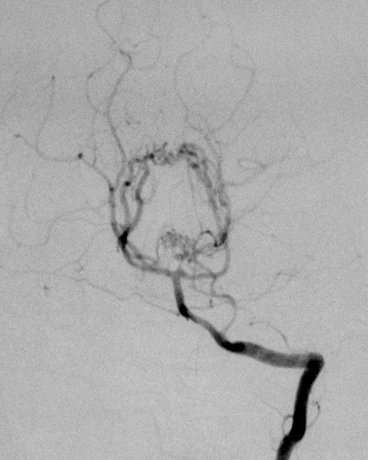
‘‘Moyamoya’’ comes from a Japanese term meaning ‘‘puff of smoke."
Describes the angiographic appearance of collateralized vessels that form in the region of the basal ganglia and beyond when radiation or other vasculopathy occludes the
internal carotid or proximal anterior and middle cerebral arteries
- Long term problem after radiation therapy especially in NF1 patients
- Progressive narrowing of the brain’s blood vessels, and obliteration of the vessels in the circle of Willis
- Occurs in up to 18% of cases