Parameningeal tumors arise in the following sites:
- Nasopharynx (most common)
- Middle ear & mastoid
- Nasal cavity & paranasal sinuses
- Infratemporal fossa including pterygoid muscle and inferior portion of temporalis muscle.
Tumors may present with:
- Sinus and nasal obstruction with a mucopurulent discharge (common).
- May be symptoms of a chronic ear infection with discharge and deafness.
- Cranial nerve palsy may indicate direct extension to the meninges. Nasopharyngeal tumors invade the base of the skull in 35% and may be associated with meningeal extension and a high risk of CNS relapse.
- Headache and vomiting can be due to raised pressure from intracranial tumor growth and erosion of the skull base.
70% are embryonal and 10% are alveolar.
Regional lymph node involvement may occur in 50%.
Patients with parameningeal tumors who have intracranial extension (direct extension into the brain) will receive radiation therapy (RT) to their primary parameningeal site ASAP at Week 1 (Day 0) (accounting for treatment planning, the actual start of RT should be within the first 2 weeks of the start of the first cycle of chemotherapy, and treatment to their metastatic sites at Week 20) .
Meningeal relapse is a real risk at this site and MR of the craniospinal axis must be part of the initial work up together with CSF cytology.
If there is leptomeningeal involvement and CSF cytology is positive, craniospinal RT is given. RT should be started as soon as possible. The dose of craniospinal RT recommended is generally 3600 cGy in 20 fractions.
Examples:
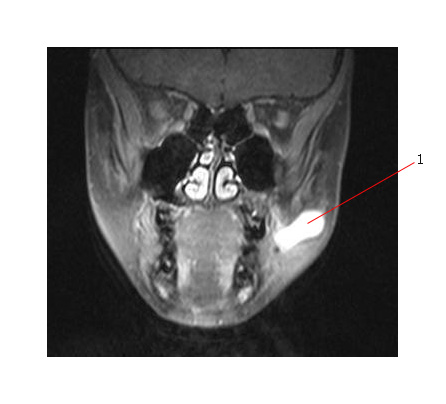
The MR scan below is of an eight year old boy and shows an alveolar RMS in the right medial extraconal space (#1). There is right sided proptosis and tumor is stretching the adjacent medial rectus muscle and immmediately adjacent to the optic nerve. There is extension into the ethmoid sinus.

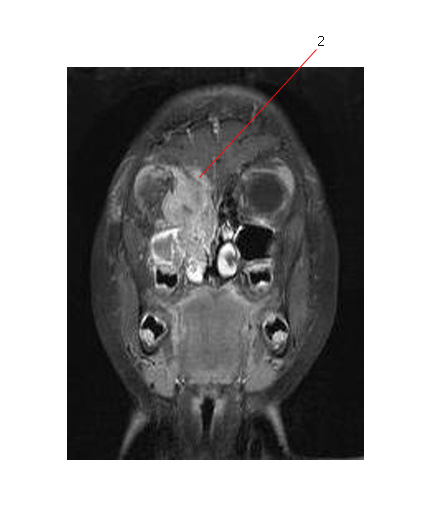
This is the same patient and the MR below shows that the tumor directly extends through the base of skull into the anterior cranial fossa (#2 points to the area where this occurs).
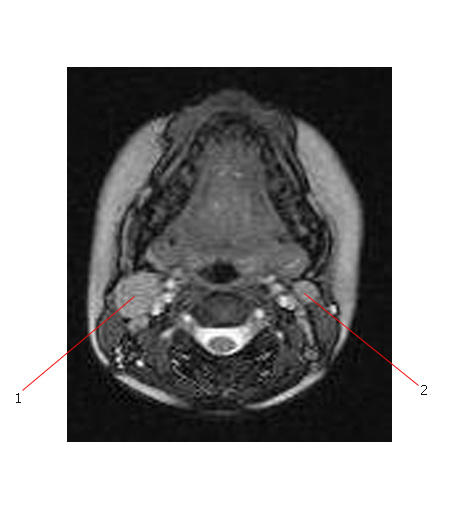
This same patient unfortunately has metastatic disease involving the cervical lymph nodes bilaterally (#1 is an ipsilateral lymph node which is more obviously involved than #2 - contralateral node - but both areas are involved by disease).
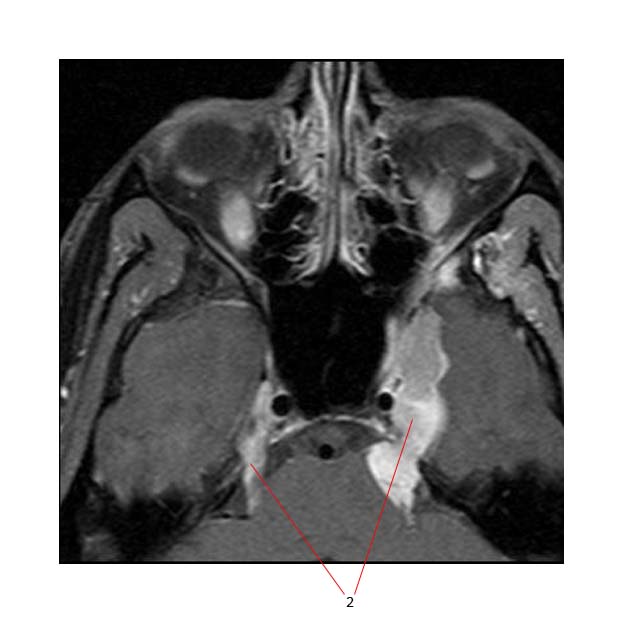
The MR below shows a rhabdomyosarcoma (1) arising in the pterygo-palatine fossa.

This was associated with extension of disease to involve the base of skull (2)
Other Head and Neck Sites
- These tend to remain localized and are often embryonal.
- Includes oral cavity, oropharynx (usually tonsil and soft palate), larynx, parotid, scalp, cheek and neck.
- Biopsy is followed by resection only if it is functionally and cosmetically possible. RT is usually required because complete excision is unusual.
- Lymph node metastases are present in about 20% of patients. Patients with positive nodes have a worse outlook. Nodes are included in the RT volume. Neck dissection and prophylactic nodal RT have not been shown to be beneficial.
Below are two MR (T2 Post gadolinium) images of the same embryonal rhabdomyosarcoma involving the cheek of a 10 year old boy (#1). The tumor probably arises from the parotid duct.