
RMS causes swelling in the affected body part (usually painless).
- Nearly 50% have alveolar histology and in this case nodal involvement is more likely. Overall there is a 20% risk of nodal metastases.
- The preferred operative procedure is wide local excision with negative margins (even to convert a patient to group II with no gross residual disease).
- Adjacent lymph node sampling (inguinal or axillary) should always be performed - even when there is no palpable abnormality
- It is important not to give RT to the entire limb circumference and a longitudinal strip of normal tissue should always be spared.
- Tumor tends to spread along fascial planes, to recur locally and to metastasize to distant sites.
- Tumors at this site have a relatively poor prognosis.
The T1 TSE coronal MR below shows an extremity RMS (#1) in a 6 year old boy:

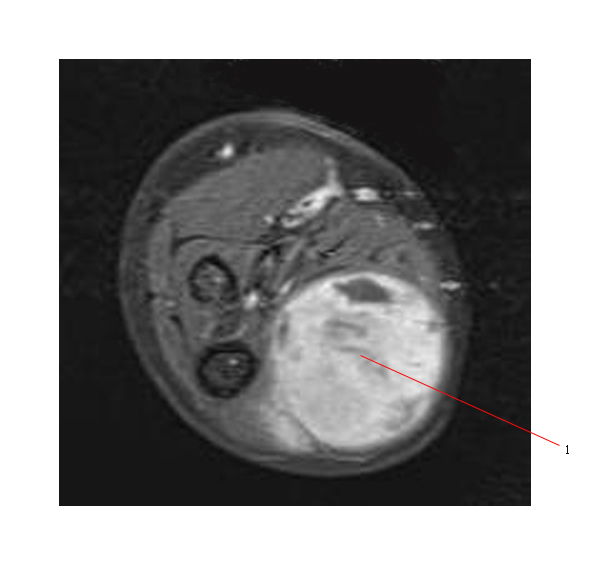
Below is a MR (Post gad transverse T1 FS) of the same tumor (#1):
Below is the PET scan of the same tumor (#1) showing increased FDG uptake:

TRUNK RMS
The prognosis is similar to extremity tumors.