
Neural crest cells give rise to the adrenal medulla, sympathetic ganglia, thyroid medullary C cells, meninges, Schwann cells, melanocytes and membranous bone.
The neural crest contains primitive stem cells which differentiate into sympathoblasts.
Neuroblastoma is most likely derived from these cells.
Origin of Neuroblastomas:
| Cells of origin | Tumor |
| Sympathoblasts | Neuroblastoma
Ganglioneuroblastoma
Ganglioneuroma |
Paraganglionic Cells |
Pheochromocytoma Paraganglioma |
Neuroblastoma is one of the "small blue round cell tumors” of childhood (others include lymphoma, Ewing sarcoma, germ cell tumors, embryonal rhabdomyosarcoma and PNETs).
There are dense nests of undifferentiated cells separated by fibrillar bundles. Haemorrage, necrosis and calcification are usually present. Tumor cells often form rosettes around a pink fibrillar center.
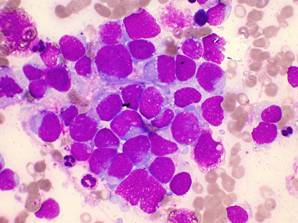
The slide below shows a bone marrow aspirate packed with neuroblastoma cells:
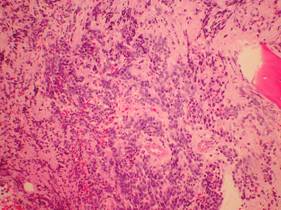
Below is a low power view of a bone marrow biopsy containing small round blue cells (again neuroblastoma).
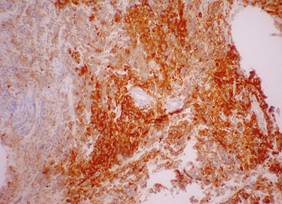
Below is a low power view of a bone marrow biopsy stained for Neuron Specific Enolase (NSE). This stain is strongly positive in neuroblastoma.
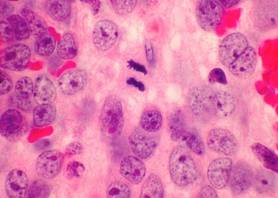
Below is a very high power view of a neuroblastoma tumor - in the middle a mitotic figure can be seen.
Ganglioneuroblastoma:
- As maturation occurs tumor cells differentiate towards ganglion cells and increasing amounts of fibrillar material are present (may not be a uniform process).
- A ganglioneuroblastoma consists of maturing or mature ganglion cells together with neuroblasts. Tumors are less aggressive than neuroblastoma.
- A ganglioneuroma is composed of well differentiated ganglion cells and is benign.
- Electron microscopy shows neurosecretory dense core granules in the peripheral cytoplasm and neural processes containing microtubules.
- Immunodiagnosis using the antibody to NSE is helpful in differentiating this tumor from other small blue cell tumors.
Neurotrophin Receptors:
- Neurotrophic factors and their receptors have been implicated in the pathogenesis of neuroblastoma.
- There is a correlation between the expression of the nerve growth factor TRKA and clinical outcome (TRKs are tyrosine kinase receptor genes).
- Tumors that had no N-myc amplification showed high TRKA expression.
- High TRKA expression was associated with 86% 5 year survival and low TRKA expression with 14% survival.
- ? TRKA and nerve growth factors cause differentiation in neuroblastoma.
Shimada index:
Shimada reviewed the pathology and his classification is used as a prognostic indicator.
- Age is taken into account.
- This has a strong prognostic significance for stages 1, 3 and 4 and 4S.
- Several criteria are used :-
- 1) Tumor is defined as being either "stroma rich" or "stroma poor". Stroma rich have more fibrillar material and therefore tend to be more mature.
- 2) Tumor cell differentiation
- 3) The nuclear morphology is evaluated by a mitosis-karyorrhexis index (MKI). The total number of mitosis and karyorrhectic cells is determined among 5000 tumor cells in randomly selected fields (less than 100 / 5000 = low and do well, more than 200 / 5000 = high).