
These patients tend to have:
- Small Stage 1 or 2 primary tumors
- Disseminated disease restricted to the liver, skin, bone marrow or any combination of these
- No skeletal involvement
The role of surgery is controversial. Generally it is agreed that the primary tumor should be removed - because there is a risk of late relapse. Surgery may take place initially or after chemotherapy.
Hepatomegaly
- The liver may become grossly enlarged leading to problems with compression of abdominal viscera, respiratory embarrassment or coagulopathy.
- May require treatment with chemotherapy or low dose RT (150 cGy x 3 doses to whole abdomen using lateral fields sparing the kidneys and ovaries).
- Neither of these treatments appear to affect survival. In a POG study chemotherapy did seem to accelerate tumor regression.
An overview of the therapy of Stage 4S is given in the low and intermediate risk NBL content sections.
Prognosis
- Some of these babies will have spontaneous resolution of their disease without treatment.
- Prognosis is generally good with 2 year survivals of 70 - 90%, regardless of treatment.
- Prognosis correlates with degree of organ compromise e.g. gastric outlet obstruction or respiratory compromise.
- Favourable subgroups within 4S are:
- 2 weeks - 12 months old
- With skin metastases, with or without liver or bone marrow involvement
- Low N-Myc amplification number
- Favourable histology
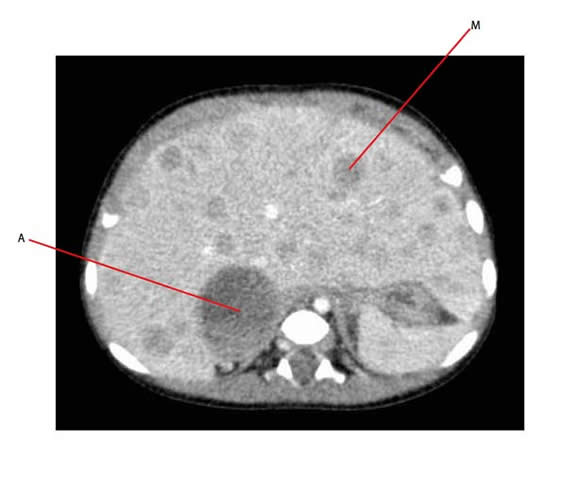
The axial CT below shows multiple metastatic nodules within the liver (M - is one of these hypodense areas) in an infant who has Stage 4S neuroblastoma. The adrenal primary is shown by A.
Below is an coronal CT of the same patient, where again A is the adrenal primary, M is one of the liver metastatic deposits and K points to the kidneys.
