
Craniospinal axis radiation therapy (CSA RT) involves treatment to the meninges surrounding the whole brain and spine. This necessarily means that the whole brain and the spine are included in the RT treatment volume.
Image to show the target volume for CSA RT:
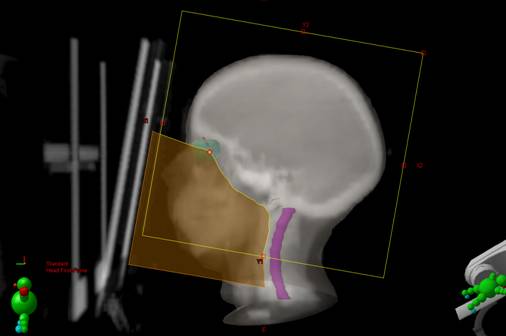
Cranial Field (prone)
In order to treat the whole brain:
- A large lateral parallel opposed pair (POP) is used:
- The collimator is rotated to match the divergence of the spinal field
- Brain fields treated at 100 cm SAD
- Brain field should extend to at least 1 cm beyond the outside of the scalp
- The fields are centered at outer canthus to minimize divergence in region of eye and cribriform plate
- The treatment field should cover the optic nerves and the cribriform plate
- The distance between the cribriform plate and the field edge should be 0.5 cm
- Shielding (multi leaf collimators or poured blocks) is used to protect the anterior portion of the orbit, the face and anterior neck
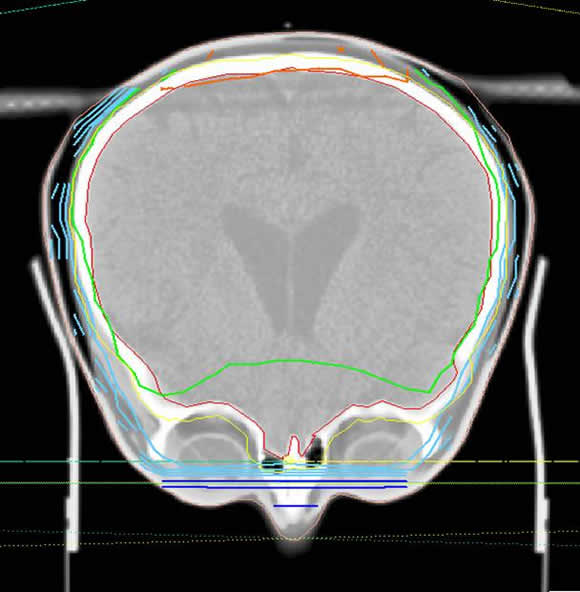
The image below shows the isodose distribution for the cranial component of CSA RT. It is possible to see that the lens are just outside the edge of the field and will receive a significant amount of scattered RT.
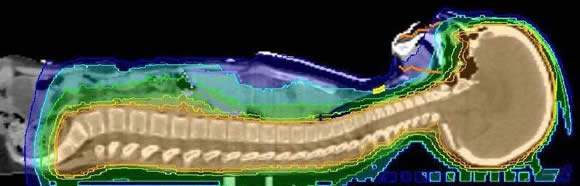
Spine Field:
The posterior spine field is set to SSD 100 cm/ 130 cm to highest midline point on spine and couch moved longitudinally to field center
Width of the spinal field should include the vertebral body with a 1 cm margin on either side (so lateral portion of theca is treated).
In the imaging below (courtesy of Dr. Roger Taylor) the CTV (clinical target volume) is in purple and the PTV (planning target volume) is in blue:
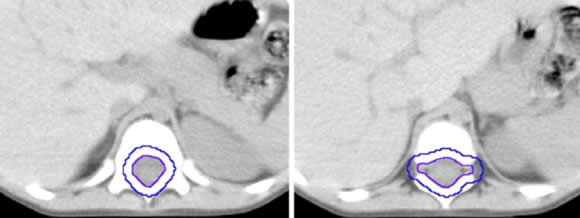
Inferior border is generally at S3/4 for a margin on the dural sac as determined by MR scan. The dural sac usually ends at S2.
The junction is accomplished by tilting the collimator of bilateral cranial fields to match the divergence of the adjacent posterior spine field.
It is best that the spine be treated with a single posterior field.
An extended SSD is preferable to the use of adjacent fields,
If 2 spinal fields have to be used then it is better that they be junctioned below L2 – inferior to the spinal cord.